
















Download the Felix App
Earn reward, visit our shop and get exclusive offers on the app
Download now
Earn reward, visit our shop and get exclusive offers on the app
Download nowPut your health first in 2026 with free visits on all categories, and $200 off longevity testing.
Download nowPut your health first in 2026 with free visits on all categories, and $200 off longevity testing.
Download now
AI-generated summaries may be inaccurate and do not constitute medical advice. Third-party AI tools are not under Felix's control, and your use of them is at your own risk.
Felix uses Levine’s Phenotypic Age, one of the most widely adopted biological age methods in north America. Felix uses Levine’s Phenotypic Age because it:
This makes it especially useful for patients doing repeat testing, lifestyle interventions, or preventative health planning. For more details, you can find the complete original publication here.
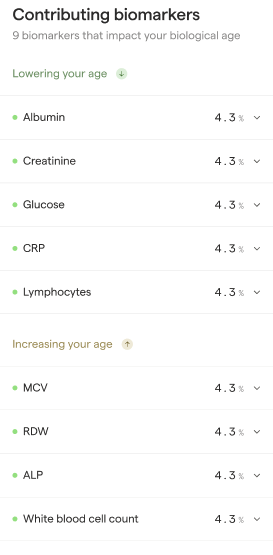
Felix reports contributing biomarkers to help patients understand what is driving their biological age result. Biological age is calculated from multiple biomarkers at once. Even if two patients have the same biological age, they may have gotten there for different reasons.
The “contributing biomarkers” feature answers:
This helps make the result actionable — rather than just a single number.
Felix uses the original NHANES III dataset that the Phenotypic Age model was derived from to understand typical biomarker distributions across age and health outcomes.
For each biomarker in the Phenotypic Age model:
Contributing biomarkers are not based on whether a value is “normal” or “abnormal” in a lab range. Rather, they’re based on whether that value pushes the Phenotypic Age model older or younger relative to the population.
This is common, and reflects the fact that biological age is model-based, not range-based.
This can happen too, because lab ranges and biological age are measuring different things.
This does not mean abnormal results should be ignored — it just means biological age isn’t meant to replace medical interpretation.
Always defer to a healthcare practitioner’s opinion over biological age.
Biological age is meant to be a helpful summary, but it’s inherently incomplete and less specific than clinical interpretation.
Because it’s based on large population studies (NHANES III), it may not account for:
Biological age is best used as:
…but it should not be treated as a diagnosis or medical advice.
Disclaimer: This blog contains links to external websites that are not provided or maintained by, or in any way affiliated with Felix. Your use of any links is at your own risk.
Appendix 1. Biological age weights
.png)
Medically reviewed by
References